Geographic Variation in the Quality and Cost of Care for Patients with Rheumatoid Arthritis
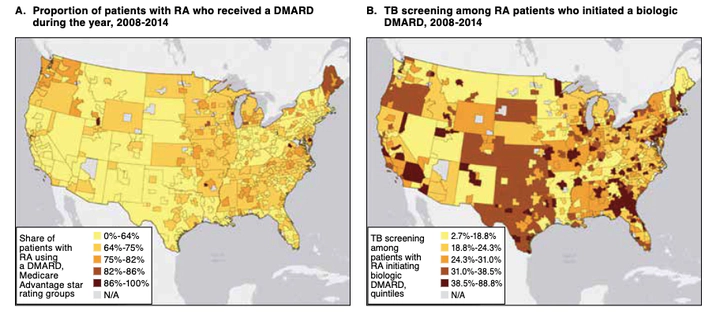 Image credit: Jinjoo Shim
Image credit: Jinjoo ShimAbstract
There is considerable push to improve value in health care by simultaneously increasing quality while lowering or containing costs. However, for diseases that are best treated with comparatively expensive treatments, such as rheumatoid arthritis (RA), there could be tension between these aims. In this study, we measured geographic variation in quality, access, and cost for patients with RA, a disease with effective but costly specialty treatments. Using large claims databases covering the period between 2008 and 2014, we measured quality of care metrics by metropolitan statistical areas (MSAs) for patients with RA. Quality measures included use of disease-modifying antirheumatic drugs (DMARDs) and tuberculosis (TB) screening before initiating biologic DMARD therapy. Access to care measures included measured detection and the share of patients with RA who visited a rheumatologist. Regression models were used to control for differences in patient demographics and health status across MSAs. For the 501,376 patients diagnosed with RA, in the average MSA 64.1% of RA patients received a DMARD, and 29.6% of RA patients initiating a biologic DMARD appropriately received a TB screening. Only 17% (73/430) of MSAs comprised the top 2 Medicare Advantage star ratings for DMARD use. Measured detection was 0.59% (IQR = 0.47%-0.71%; CV = 0.355) on average, and 57.6% (IQR = 48%-69%; CV = 0.341) of RA patients visited a rheumatologist. MSAs with the highest DMARD use spent $26,724 (in 2015 U.S. dollars) annually treating patients with RA, $5,428 more (P < 0.001) than low DMARD-use MSAs, largely because of higher pharmacy cost ($5,090 vs. $7,610, P < 0.001). However, MSAs with higher DMARD use had lower RA-related inpatient cost ($1,890 vs. $2,342, P = 0.024). There were significant geographic variations in the quality of care received by patients with RA, although quality was poor in most areas. Fewer than 1 in 5 MSAs could be considered high quality based on patient DMARD use. Access to specialist care may be an issue, since just over half of patients with RA visited a rheumatologist annually. Efforts to incentivize better quality of care holds promise in terms of unlocking value for patients, but for some diseases, this approach may result in higher costs.
Jinjoo Shim
Digital Health Data Scientist
My research interests is to advance digital healthcare through AI/ML and data science.